Thoraco-Coraco-Pectoral Space
Several issues related to the thoraco-coraco-pectoral (TCP) space can exacerbate symptoms of thoracic outlet syndrome (Hooper et. al., 2010). Thus, a multifaceted approach is recommended to improve the likelihood of reducing symptoms.
Shortening of the pectoralis minor or pectoralis major muscles can cause narrowing of the TCP space (Hooper et. al., 2010).
- Soft tissue mobilization and stretching of these muscles may reduce pressure on the brachial plexus.
Patients with narrowing of the TCP space often present with a forward head posture and rounded, sagging shoulders (Hooper et. al., 2010).
- Postural awareness and correction, including encouraging a relative retraction of the shoulders, will increase the TCP space.
- A strip of elastic therapeutic tape applied across the scapula while the patient is in a comfortably retracted posture provides tactile cuing to help prevent the patient’s shoulders from falling into a protracted position.
- A supportive bra with wide, crossed posterior straps may help to reduce sagging shoulders in women with heavy breasts.
Aberrance in scapular mechanics due to compromised control of shoulder girdle musculature is often implicated in the development or progression of TOS (Hooper et al, 2010, Watson et. al., 2010).
- Sensorimotor control exercises for the rhomboids, serratus anterior, and lower and middle trapezius muscles should be initiated in a gravity-assisted position to facilitate recruitment of lower scapular stabilizers and reduce the influence of upper scapular elevators (Novak, 2003).
- Exercises should focus on muscular endurance rather than strength (Novak, 2003).
Tension and adhesion formation may develop in response to a loss of neural mobility (Hooper et. al., 2010).
- Neural mobilization involving gliding of the neural tissue in relation to its surroundings is especially important in cases of a double crush phenomenon.
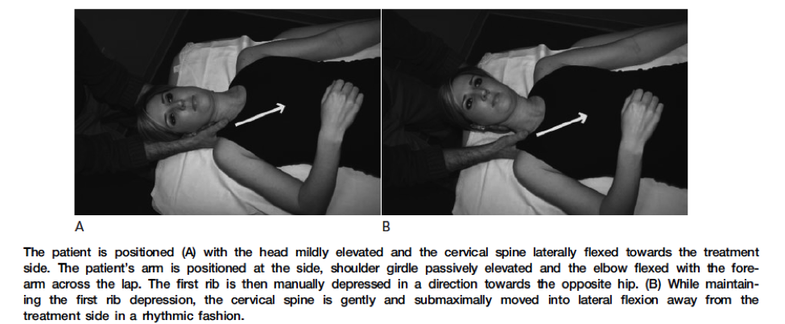
- Techniques can be modified for focus on the brachial plexus proximally in the costoclavicular or TCP space while the clinician performs an inferior mobilization of the first rib as follows:
Proximal Neural Mobilization